778
Views & Citations10
Likes & Shares
Objective: To investigate the frequency of usage of
areca nut among rural population and to mark the deleterious effects on health
among the areca nut chewers.
Methods: The concern studies have glared the
deleterious effect of chewing areca nut on oral health. Data was collected with
the pre-structured questionnaire among 707 study participants. Chi square test
of significance was used for data analysis.
Results: Among the study participants 67.01% have the
habit of chewing betel leaf with areca nut along with other constituents. This
is nearly of about areca nut chewers, i.e., 32.99%. The study illustrates the
strong association between the habit of chewing areca nut/betel leaf/areca nut
with other constituents and with the development of oral lesion. Areca nut
chewers (3.28%) have more pervasiveness over the combination of betel leaf,
areca nut with other constituents (2.69%) in the age group of less than 25
years.
Conclusion: Areca nut and its compounds have deleterious
effect on oral mucosa. Strict prohibition should be implemented to inhibit the
ease of availability. Health warnings should be highlighted with the legal prohibition
to turn down the spread of oral lesion.
Keywords: Areca nut, Betel leaf, Oral lesion, Rural
population
INTRODUCTION
Quid is a
substance or mixture of substances (in any manufactured or processed form) that
is placed in the mouth, where it is sucked or actively chewed and thus
remains in contact with the mucosa over an extended period. It usually contains
one or both of 2 basic ingredients, tobacco and areca nut [2]. The composition
of betel quid, also known as paan, varies between communities and individuals, although the major constituents are areca nut and slaked lime (from limestone or coral) wrapped within a betel leaf. The paan is placed between the teeth and the buccal mucosa and is gently chewed or sucked over a period
of several hours [2,3]. The slaked lime acts to release an alkaloid from the
areca nut, which produces a feeling of euphoria and well-being [4]. Other substances
of local preference may be added, such as grated coconut or a variety of
spices, for example, aniseed,
peppermint, cardamom and cloves [5]. Ingredients of paan (sliced areca nut wrapped in betel leaf) are added according
to personal preferences. In addition, the lime has been shown to release
reactive oxygen species from extracts of areca nut, which might contribute to
the cytogenetic damage involved in oral cancer. Variants of pan include use of sliced areca nut
alone and addition of sweeteners to make the
product particularly attractive to buyer, to whom it is sold under the name sweet supari,
gua, mawa or mistee pan [3,6].
It is used by men and women—in some societies
the latter predominate. All age groups and social classes use the product.
Areca nut has a long history of use and is deeply ingrained in many
sociocultural and religious activities [7].
Arecoline has been isolated from the basic
nut [8] and has major effects on various neurotransmitters particularly on
cholinergic neurones, but there are a variety of other alkaloids—namely, arecaidine,
guracine, guacine and arecolidine, as well as unidentified peaks on
chromatography of the extracts.
Chewing areca nut on a habitual basis is
known to be deleterious to human health [9]. A growing body of evidence over
the last 40 years, mainly in the form of large-scale epidemiological and
experimental studies, has shown that even when consumed in the absence of tobacco or lime areca may have potentially harmful
effects on the oral cavity. The study upholds the deleterious effect of chewing
areca nut on oral health.
MATERIALS AND METHODS
The present cross-sectional study was
conducted among the rural population. Villages 50-60 km away from New Delhi are
included in the study. The study was conducted from January to June 2018.
Purposive sampling was adopted for choosing the rural population, as some
cultural customs are prevalent among the
specific group of population. The villagers were informed about the health
check camps for next few days. This was done to engulf the
maximum number of populations in the concern study. Total 707 people attended
people attended the camp and accounted for the
sample size. Total of 15-20 individuals were interviewed daily on basis of
pre-structured and pre-designed questionnaire by the principal investigator.
The individuals with clinical lesions were than stained with Toludine blue
(colorizing agent) and acetic acid (decolorizing agent) with appropriate
aseptic technique for diagnosing the cases of oral lesion. Data was collected
with the pre-structured questionnaire including the habit of consumption of
areca nut and its different compounds.
RESULTS
Friends and
family may be among the first to recognize the Betel leaf, areca nut chewers with other
components (like tobacco, slake-lime, etc.) and Areca nut chewers with other
flavonoids are smokeless form of tobacco. They are prevalent among villagers as
areca nut chewers and betel leaf chewers are not easily noticed. Total village
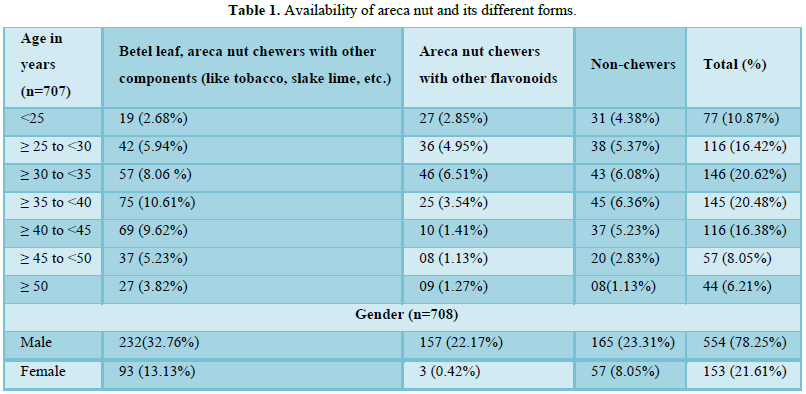
population examined 67.01% have the habit of chewing areca nut with betel leaf
or with any other flavonoids.
Areca nut is
cut from areca nut cutter and it is chewed
accordingly, 32% of the study participants chew areca nut with other
flavonoids. The study shows ease of
availability of areca nut and its different forms (Table 1).
Study participants in the age range 30-40
years have the habit of chewing areca nut with or without betel leaf. This may
be due to cultural and social acceptance or may be due to peer group
involvement in the habit of chewing. Social gathering offer areca nut with or without betel leaf as a mark
or token of greet.
The study submits the male predilection for
the habit of chewing areca nut in any form. It was observed (3.6:1) among total
populations. The younger population is consuming more areca nut with other
flavonoids as compare to the chewing habit of betel leaf in combination with
areca nut, slake-lime and other compounds. This may be the crude cause of
mortality due to complications of premalignant lesions among youngsters. There
may be possibility of easy availability, at a low price, with good fragrance
that the younger generation is fond of areca nut related compounds. Khandelwal
et al. have illustrated the early usage of areca-nut among adolescents.
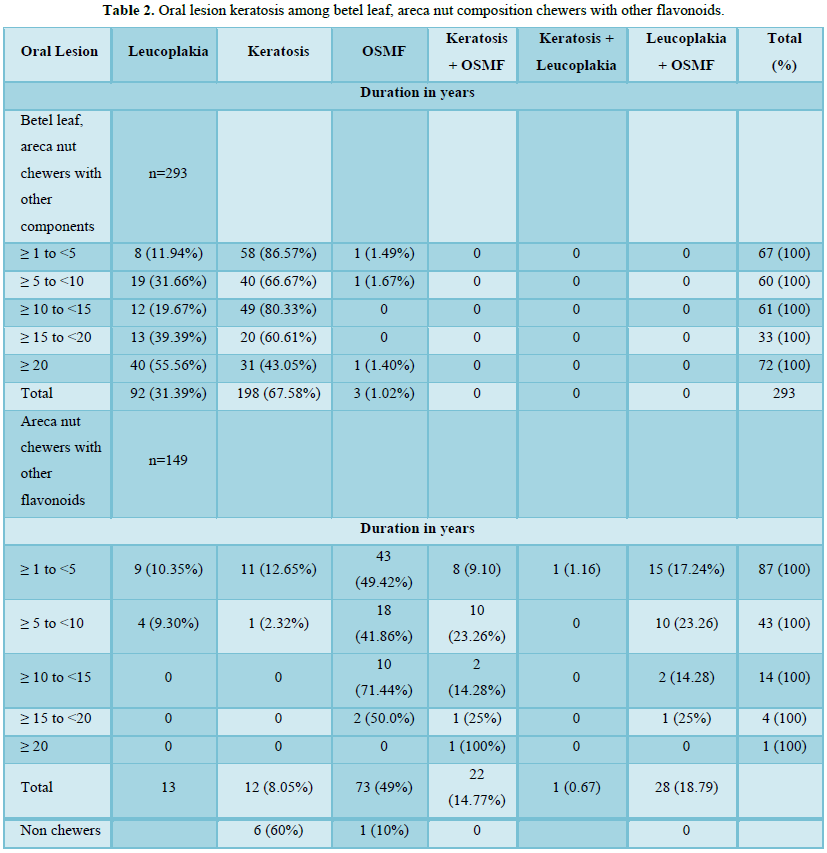
Oral lesion keratosis accounted at 67.58% and
8.05% among betel leaf, areca nut composition chewers and areca nut chewers
with other flavonoids (Table 2).
Maximum of
86.5% of areca nut in betel leaf chewers with other components had the
keratosis lesion within five years. (Table
2). Prevalence of OSMF among the villagers with the habit of chewing betel
leaf along with areca nut and another components population was estimated at
18.89%.
Areca nut with other flavonoids chewers has
demonstrated the maximum OSMF 49% (Table
2). The overall prevalence of leucoplakia in the present study is estimated
at 15.27%. This premalignant condition was observed in 31.40% and 8.72% among
combination of areca nut, betel leaf with other components and areca nut with
other flavonoids, respectively (Table 2).
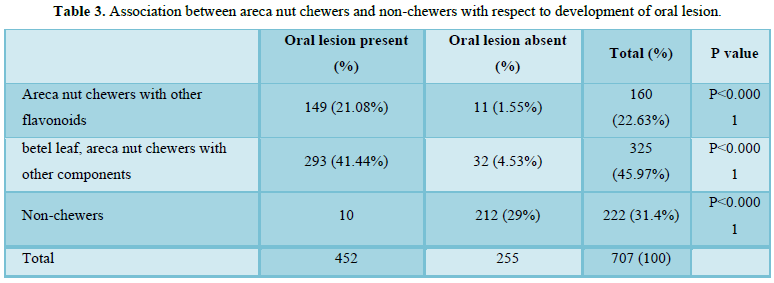
The association between Areca nut chewers
with other flavonoids, betel leaf (combination with areca nut and other
components) and non-chewers with respect to development of oral lesion was
highly significant (Table 3).
DISCUSSION
Areca nut is
the fourth most commonly used substance of abuse in the world after tobacco,
alcohol and caffeine. Areca nut is psychoactive substance used by millions of
people in India and world-wide [10]. Areca nut is easily accessible among the
villagers; it is cost effective and least noticed.
Studies have confirmed the addictive
ingredients in areca nut [11]. Arecoline
is
a main carcinogenic component in areca nut [12]. There is good evidence that supports the role of areca nut chewing enhance the risk of
OSMF. Studies have illustrated that alkaloids from areca nut such as arecoline
and its hydrolysed product arecaidine may stimulate cultured fibroblasts to
proliferate and synthesize collagen [13,14]. In addition flavonoids within the
nut have also been shown to increase the stabilization of collagen by enhancing
the cross-linking of collagen, thereby increasing the resistance to degradation
by collagenases [15]. Furthermore, recent studies have shown that arecoline inhibits collagen synthesis and fibroblast
proliferation in vitro, suggesting
that arecoline may have cytotoxic properties
[16-18].
Chewing areca
nut with betel leaf is very prevalent among the study participants. The pan is
sucked or chewed which provide the addictive feeling of euphoria. The data
suggest that the habit of chewing betel leaf with areca nut increases the risk
of developing oral lesion [19].
Areca nut with
betel leaf (pan) chewing without tobacco causes oral cancer have been
highlighted in a few recent studies. According to Van Wyk et al. [20], 68% of
cheek cancers and 84% of tongue cancers were found in subjects consuming areca
without tobacco. Furthermore, there is new evidence which suggest that areca in
the absence of tobacco may be an independent risk factor for the development of
oral cancer [21].
Chewing
habitual areca nut leads incisal and cuspal grinding of the teeth with leads to
the loss of enamel and exposure of underlying dentine. There may be high
incidence of root fracture due to increase masticatory force among areca nut
chewers [22].
Studies have
suggested that areca nut chewers have less feasibility of dental caries as
compare to the non-chewers [23-25]. Stains among areca nut chewers often coat
the tooth surface, which act as a protective varnish [26]. Studies have
suggested that tannin content of areca nut may have anti-microbial properties
and this may contribute to the cariostatic role of areca nut [27]. Habitual
chewing may result in incisal and cuspal grinding, which may reduce the risk of
pit and fissure caries by eliminating the potential stagnation areas.
Attrition leads
to the increased production of sclerosed dentine, thus countering the microbial
invasion. Areca nut chewing lead to the production of abundant amount of
saliva, presence of slake lime may increase the pH in oral environment; this
may act as a buffer against the acid formed in plaque on teeth.
CONCLUSION
The role of
areca nut and its different form have been strongly associated with oral
lesion. Contribution of areca nut and its different forms in oral lesion
highlights the importance of public health education. These products are
inadequately labeled. They are no health warnings labels and no restriction on
its sale to children or consumption on public places.
Areca nut usage
is culturally bound and is an integral aspect of several Indo-Asian customs and
thus part of their identity. Casual use of small quantities of areca nut on a
non-regular basis is widely prevalent in Asian communities.
Although this
practice is unlikely to have long term ill effects with time, some individuals
may develop a dependency syndrome. In certain communities the preparation and
sale of areca products makes a significant financial contribution to the local
economy. Accurate labelling of the products, especially with respect to
admixture with tobacco, should be an important requirement. Health warnings
should be enacted, but outright bans or restriction will probably prove to be
counterproductive.
1. Gupta PC, Warnakulasuriya S (2002)
Global epidemiology of areca nut usage. Addict Biol 7: 77-83.
2. Zain RB, Ikeda N, Gupta PC, Warnakulasuriya
KAAS, van Wyk CW, et al. (1999) Oral mucosal lesions associated with betel
quid, areca nut and tobacco chewing habits: Consensus from a workshop held in
Kuala Lumpur, Malaysia, 25-27. J Oral Pathol Med 28: 1-4.
3. Farrand P, Rowe RM, Johnston A,
Murdoch H (2001) Prevalence, age of onset and demographic relationships of
different areca nut habits amongst children in Tower Hamlets, London. Br Dent J
190: 150-154.
4. Neville BW, Damm DD, Allen CM,
Bouquot JE (2002) Oral and maxillofacial pathology. 2nd Edn.
Philadelphia: W.B. Saunders Company, pp: 349-350.
5. International Agency for Research
on Cancer (1985) IARC monographs on the evaluation of the carcinogenic risk of
chemicals to humans. Tobacco habits other than smoking; betel-quid and
areca-nut chewing; and some related nitrosamines. Lyon, France: IARC, p: 291.
6. Shah B, Lewis MA, Bedi R (2001)
Oral sub mucous fibrosis in an 11 year old Bangladeshi girl living in the
United Kingdom. Br Dent J 191: 130-132.
7. Williams SA (1995) Betel-quid
chewing: A community perspective. In: Bedi R, Jones P, eds. Betel-quid chewing
among Bangladeshi community in the United Kingdom. London: Centre for
Transcultural Oral Health, pp: 11-25.
8. Arjungi von KN (1976) Areca nut.
Arzneim-Forsch (Drug Res) 26: 951-956.
9. Trivedy C, Warnakulasuriya S,
Peters TJ (1999) Areca nuts have deleterious effects. Br Med J 318: 1287.
10. International Agency for Research
on Cancer: IARC (1984) Monographs on the evaluation of the carcinogenic risk of
chemicals to humans. Tobacco habits other than smoking; betel-quid and areca
nut chewing; and some related nitrosamines. Lyon: International Agency for
Research on Cancer, p: 37.
11. Lord GA, Lim CK, Warnakulasuriya
S, Peters TJ (2002) Chemical and analytical aspects of areca nut. Addict Biol
7: 99-102.
12. Hoffmann D, Rivenson A,
Prockopczyk B (1992) Advances in tobacco carcinogenesis. Smokeless tobacco and
betel quid. In: Gupta PC, Hamner JE III, Murti PR, editors. Control of
Tobacco-Related Cancers and Other Diseases. Bombay: Oxford University Press,
pp: 193-204.
13. Canniff JP, Harvey W (1981) The
etiology of oral sub mucous fibrosis: The stimulation of collagen synthesis by
extracts of areca nut. Int J Oral Surg 10: 163-167.
14. Harvey W, Scutt A, Meghji S,
Canniff JP (1986) Stimulation of human buccal mucosa fibroblasts in vitro by
betel-nut alkaloids. Arch Oral Biol 31: 45-49.
15. Scutt A, Meghji S, Canniff JP,
Harvey W (1987) Stabilisation of collagen by betel nut polyphenols as a
mechanism in oral sub mucous fibrosis. Experientia 43: 391-393.
16. Chang MC, Kuo MY, Hahn LJ, Hsieh
CC, Lin SK, et al. (1998) Areca nut extract inhibits the growth, attachment and
matrix protein synthesis of cultured human gingival fibroblasts. J Periodontol
69: 1092-1097.
17. van Wyk CW, Olivier A, de Miranda
CM, van der Bijl P, Grobler-Rabie A (1994) Observations on the effect of areca
nut extracts on oral fibroblast proliferation. J Oral Pathol Med 23: 145-148.
18. Jeng JH, Lan WH, Hahn LJ, Hsieh
CC, Kuo MY (1996) Inhibition of the migration, attachment, spreading, growth
and collagen synthesis of human gingival fibroblasts by arecoline, a major
areca alkaloid, in vitro. J Oral
Pathol Med 25: 371-375.
19. Thomas S, Wilson A (1993) A
quantitative evaluation of the etiological role of betel-quid in oral
carcinogenesis. Eur J Cancer Oral Oncol 29B: 265-271.
20. van Wyk CW, Stander I, Padayachee
A, GroblerRabie AF (1993) The areca nut chewing habit and oral squamous cell
carcinoma in South African Indians. A retrospective study. S Afr Med J 83:
425-429.
21. Merchant A, Husain SS, Hosain M
(2000) Paan without tobacco: An independent risk factor for oral cancer. Int J
Cancer 86: 128-131.
22. Yeh CJ (1997) Fatigue root
fracture: A spontaneous root fracture in non-endodontically treated teeth. Br
Dent J 182: 261-266.
23. Moller IJ, Pindborg JJ, Effendi I
(1977) The relation between betel chewing and dental caries. Scand J Dent Res
85: 64-70.
24. Schamschula RG, Adkins BR, Barmes
DR, Charlton G (1977) Betel chewing and caries experience in New Guinea.
Community Dent Oral Epidemiol 5: 284-286.
25. Nigam P, Srivastava AB (1990)
Betel chewing and dental decay. Fed Oper Dent 1: 36-38.
26. Howden GF (1984) The cariostatic
effects of betel chewing. PNG Med J 27: 123-131.
27. de Miranda CM, van Wyk CW, van der
Biji P, Basson NJ (1996) The effect of areca nut on salivary and selected organisms.
Int Dent J 46: 350-356.
-
 Table 1
Table 1 -
Table 2
-
Table 3
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Allergy Research (ISSN:2642-326X)



